Free 3-5 day delivery
on all orders

Cat is positioned in lateral recumbency with the affected side uppermost.
Cat is under anaesthesia and clipped/draped as per an aseptic procedure.

Local anaesthetic (e.g. Bupivacaine) is a good idea even though the drain is temporary.
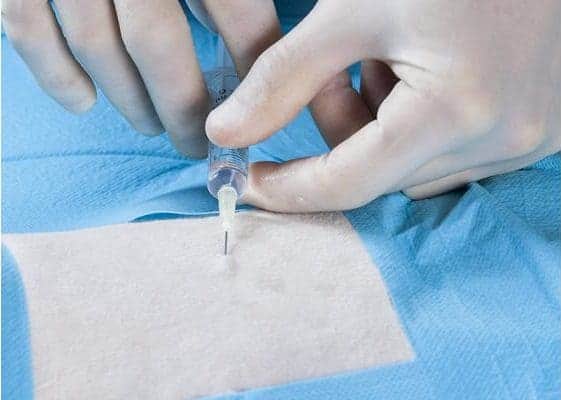
Local anaesthetic is injected at the site of drain placement (1-2mg/kg). Run cutaneously and cranially in a 2cm tunnel at the 10th intercostal space.

A stab incision is made in the skin.

Drain ready for insertion. Note the marks on the side to indicate the depth of insertion. The tip of the trochar has a pyramidal point and this must protrude from the drain tip during the procedure.

Drain placed in stab incision and inserted in a cranial direction sub-cutaneously.

Drain is lifted vertically; the tip is positioned over the middle of the intercostal space (typically 7th or 8th).

Drain is inserted with a thrusting action 1cm or so into the pleural space with the fingers controlling the depth of penetration.

The drain is then laid flat and advanced further whilst holding the trocar in a fixed position.

Drain is inserted up to the hub.

Aspiration or air or fluid by means of a connected syringe will confirm appropriate placement.

A three-way tap can be used for continual drainage.

Fluid can be withdrawn and then expressed through the tap by changing the position of the valve on the tap.

For larger volumes of fluid an extension set can be connected to the sidearm which reduces the aerosol effect and general contamination.

A centesis valve can be connected to the drain. Aspiration is carried out through one arm of the tap and then expressed through a sidearm.

Using a syringe with a centesis valve.

A mini Heimlich valve can be used as a convenient one-way valve.

A slightly larger thoracic trocar suitable for the cat. Again placed through a subcutaneous tunnel.

The trocar is lifted vertically and pushed firmly down to insert into pleural space. The tip of the trocar is protruding from the end of the drain at all times.

Fingers controlling the depth of penetration.

Once inserted, remove the trocar.

A standard luer-lock connection once the trocar has been removed.







